Fill in Your Care 1St Arizona Prior Authorization Form
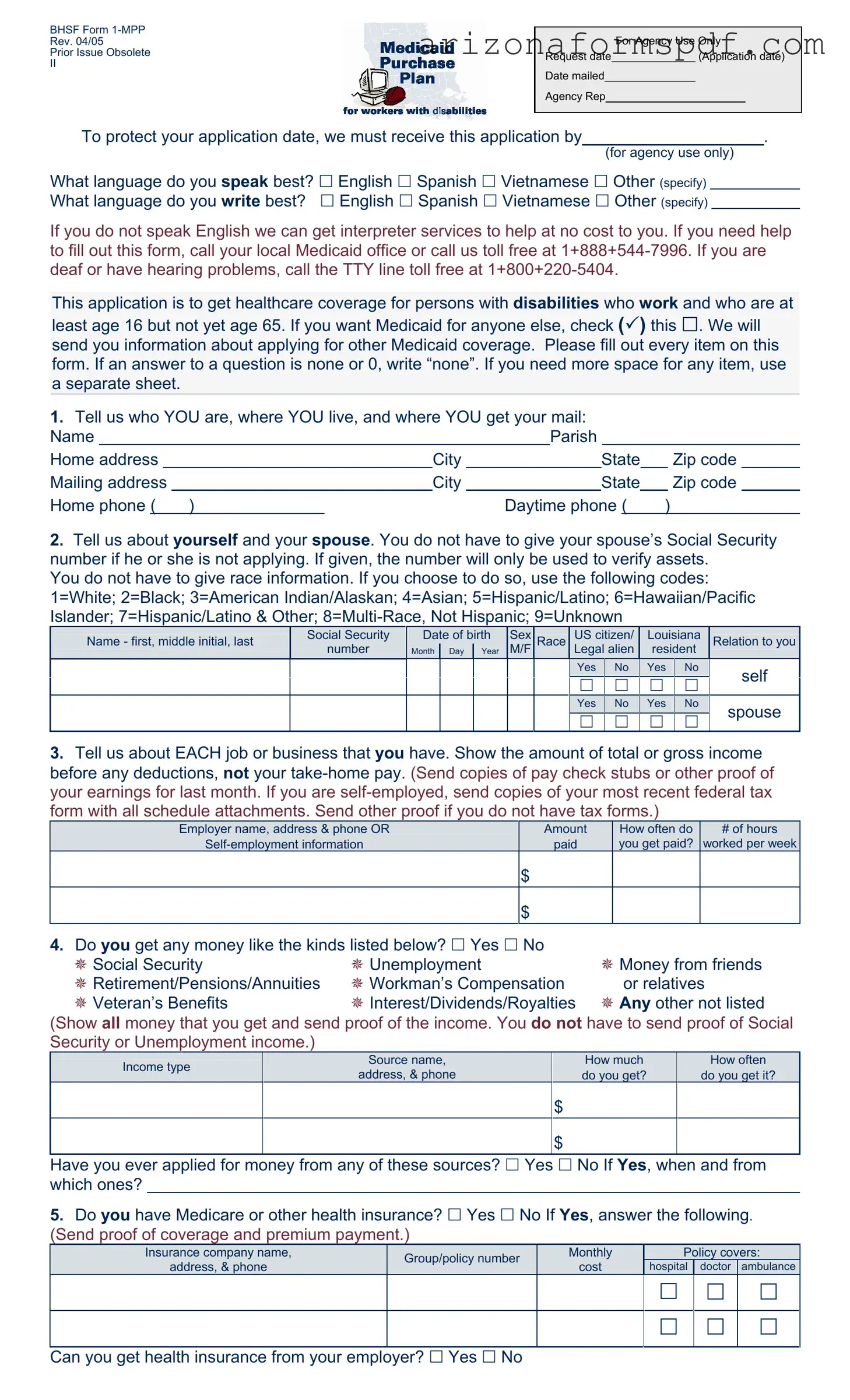
The Care 1st Arizona Prior Authorization Form serves a crucial role in the process of accessing healthcare services for individuals with disabilities who are employed and aged between 16 and 65, seeking Medicaid coverage. This comprehensive form, outlined as BHS/\F Form 1-MPP and revised last in April 2005, addresses various key areas necessary for application. It starts by inquiring about basic personal information, extending to details about one’s spouse, employment, and any other sources of income, thus painting a holistic picture of the applicant's financial status. Additionally, it probes into the applicant's health insurance status, assets, and resources to ensure a thorough assessment for eligibility. Pertinently, the form touches upon the applicant's disability, requiring detailed information about medical care providers, which emphasizes the focus on tailoring healthcare coverage to the individual’s specific needs. Furthermore, it underlines the importance of honest and accurate information submission, recognizing its significance in the eligibility determination process. This form not only serves as an application but also as a declaration of the applicant's responsibilities and rights, including understanding the consequences of fraudulent information, the necessity of cooperation in eligibility verification, and the agreement to report changes that might affect coverage. Lastly, it reassures applicants of their right to fair treatment and the availability of a Fair Hearing should they dispute the decisions made regarding their application, underscoring a commitment to justice and equal access to healthcare services.
Document Preview
BHSF Form
Rev. 04/05
Prior Issue Obsolete
II
For Agency Use Only
Request date |
|
(Application date) |
Date mailed
Agency Rep
To protect your application date, we must receive this application by |
|
. |
(for agency use only)
What language do you speak best? English Spanish Vietnamese Other (specify) What language do you write best? English Spanish Vietnamese Other (specify)
If you do not speak English we can get interpreter services to help at no cost to you. If you need help to fill out this form, call your local Medicaid office or call us toll free at
This application is to get healthcare coverage for persons with disabilities who work and who are at
least age 16 but not yet age 65. If you want Medicaid for anyone else, check ( ) this . We will send you information about applying for other Medicaid coverage. Please fill out every item on this form. If an answer to a question is none or 0, write “none”. If you need more space for any item, use a separate sheet.
1.Tell us who YOU are, where YOU live, and where YOU get your mail:
Name |
|
|
|
Parish |
|
|
|
|
||||||
Home address |
|
City |
|
|
State |
|
Zip code |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing address |
|
City |
|
|
State |
|
Zip code |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||
Home phone ( ) |
|
Daytime phone ( |
) |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2.Tell us about yourself and your spouse. You do not have to give your spouse’s Social Security number if he or she is not applying. If given, the number will only be used to verify assets.
You do not have to give race information. If you choose to do so, use the following codes: 1=White; 2=Black; 3=American Indian/Alaskan; 4=Asian; 5=Hispanic/Latino; 6=Hawaiian/Pacific Islander; 7=Hispanic/Latino & Other;
Name - first, middle initial, last |
Social Security |
Date of birth |
Sex |
Race |
US citizen/ |
Louisiana |
Relation to you |
||
|
number |
Month |
Day |
Year |
M/F |
|
Legal alien |
resident |
|
|
Yes |
|
No |
|
Yes |
|
No |
|
self |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|||||||
|
Yes |
|
No |
|
Yes |
|
No |
|
spouse |
|
|
|
|
|
|
||||
3.Tell us about EACH job or business that you have. Show the amount of total or gross income before any deductions, not your
Employer name, address & phone OR |
Amount |
How often do |
# of hours |
paid |
you get paid? |
worked per week |
$
$
4.Do you get any money like the kinds listed below? Yes No
Social Security |
Unemployment |
Money from friends |
Retirement/Pensions/Annuities |
Workman’s Compensation |
or relatives |
Veteran’s Benefits |
Interest/Dividends/Royalties |
Any other not listed |
(Show all money that you get and send proof of the income. You do not have to send proof of Social Security or Unemployment income.)
|
Income type |
|
Source name, |
|
|
How much |
|
How often |
|
|
|
address, & phone |
|
|
do you get? |
|
do you get it? |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
$ |
|
|
|
|
$
Have you ever applied for money from any of these sources? Yes No If Yes, when and from which ones?
5.Do you have Medicare or other health insurance? Yes No If Yes, answer the following. (Send proof of coverage and premium payment.)
Insurance company name, |
Group/policy number |
Monthly |
|
Policy covers: |
|||
address, & phone |
cost |
hospital |
doctor |
ambulance |
|||
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Can you get health insurance from your employer? Yes No
6.Do you, or you jointly with your spouse, have any assets or resources like those listed below? Yes No If Yes, give us the following information. (Send proof of ownership and value.)
|
Asset/Resource |
Company name, address, & phone; |
Value |
Amount owed |
|
||||
|
Account number and/or description |
|||
|
|
|
|
|
|
Checking/Savings accounts (type) |
|
$ |
|
|
|
|
|
|
|
Certificates of Deposit |
|
$ |
|
|
Retirement accounts |
|
$ |
|
|
Annuities/Trusts |
|
$ |
|
|
Stocks/Bonds |
|
$ |
|
|
Vehicles (if more than one) |
|
$ |
$ |
|
Property, other than your home |
|
$ |
$ |
|
Other (please be specific) |
|
$ |
$ |
7.Did you ever apply for or get Social Security Disability or Supplemental Security Income (SSI)
benefits? Yes No If Yes, when? |
|
Was a decision made? Yes No |
|
If Yes, what was the decision? |
|
|
|
|
|
|
|
8.What is your disability?
Tell us about the doctors or other medical providers who care for you:
Provider’s name(s)
Address & phone of this medical provider
9.Where did you find out about the Medicaid Purchase Plan?
Rights and Responsibilities
I declare that I am a U.S. citizen or in this country legally.
The information I gave on this form is true and correct to the best of my knowledge. I realize if I knowingly give information that is not true OR if I knowingly hold back information, I may get health benefits for which I am not eligible. If that happens, I can be lawfully punished for fraud. I may also have to pay Medicaid back for any medical bills which are paid incorrectly.
I understand that the information I give about my situation will be checked. I agree to help do that, and to let Medicaid get information it needs from government agencies, employers, medical providers, and other sources. If I refuse to help with this process or in later reviews caused by reported changes, or as part of a Recipient Eligibility review, it will mean that I can’t get Medicaid until I do help.
I know that Social Security numbers will only be used to get information from other government agencies to prove my eligibility.
I agree to tell Medicaid within 10 days if 1) I move out of state; 2) there are changes in where I live or get my mail; 3) there are any changes in other health insurance coverage; 4) there is any change in my work status.
By accepting Medicaid, I agree that any medical payments received from other sources will be sent to the Department of Health and Hospitals for any services that were covered by Medicaid.
I can ask for a Fair Hearing if I think the decision made on my case is unfair, incorrect or being made too late.
Medicaid can’t treat me differently because of my race, color, sex, age, disability, religion, nationality or political belief. If I think they have, I can call the U.S. DHHS Regional Office for Civil Rights in Dallas, TX at
Signature of Applicant or Authorized Representative |
|
Date |
|
|
|
Signature of Agency Representative, if applicable |
|
Date |
File Properties
| Fact Number | Description |
|---|---|
| 1 | This form is meant for individuals with disabilities who are working, aged 16 to 64, seeking Medicaid coverage. |
| 2 | Applicants are not required to disclose their race or their spouse's Social Security number unless the spouse is also applying. |
| 3 | The form supports multilingual applicants, offering services in English, Spanish, Vietnamese, and other languages upon specification. |
| 4 | There are provisions for interpretation services at no cost to the applicant if they do not speak English. |
| 5 | Applicants must provide detailed information about their income, including employment, self-employment, and any other sources of income. |
| 6 | There is a requirement to disclose assets and resources, highlighting the need for proof of ownership and value. |
| 7 | The form has a section devoted to rights and responsibilities, underlining the importance of providing truthful information and the consequences of not doing so. |
Instructions on Writing Care 1St Arizona Prior Authorization
Filling out the Care 1St Arizona Prior Authorization form is a straightforward process that ensures you get the necessary healthcare coverage efficiently. It's a document designed for individuals with disabilities who are employed, aged between 16 and 65, looking to apply for healthcare coverage. Remember, accuracy and honesty are crucial when completing this form to avoid any possible delays or issues with your application. Follow these steps meticulously to ensure a smooth submission process.
- Under the section "For Agency Use Only", leave it blank as it will be filled out by the agency representative.
- In the question about language proficiency, check the box that corresponds to the language you speak and write best (English, Spanish, Vietnamese, or specify another if applicable).
- If you are not fluent in English and require interpreter services, remember that the form mentions assistance is available at no cost.
- For any help filling out the form, note the provided contact numbers but proceed to fill out personal and contact details as follows:
- Enter your full name, home address, city, state, and zip code in the designated spaces.
- Provide your mailing address if different from your home address.
- List both your home phone number and a daytime phone number.
- When detailing information about yourself and your spouse, remember you're not required to provide a Social Security number for a non-applying spouse. Choose to provide race information only if comfortable, using the listed codes.
- Describe each job or business you have, including employer details or self-employment information. Indicate your gross income, frequency of payment, and the average number of hours worked per week. Attach necessary proof of earnings as instructed.
- If you receive any other types of income, such as Social Security, unemployment, etc., check "Yes" and detail the source, amount, and frequency of each. Indicate whether you've applied for these sources before if applicable.
- Answer whether you have Medicare or other health insurance. If "Yes," include the required details about your insurance coverage and remember to attach proof of coverage.
- Disclose any assets or resources you or your spouse own, detailing type, company name, value, and amount owed if applicable. Attach proof of ownership and value as directed.
- Indicate if you've ever applied for or received Social Security Disability or Supplemental Security Income (SSI) benefits, including dates and decisions made on those applications.
- Describe your disability and provide information about your medical providers to support your application.
- Indicate how you learned about the Medicaid Purchase Plan.
- Review the Rights and Responsibilities section carefully. By signing the form, you affirm that all information provided is accurate and understand the implications of providing false information.
- Sign and date the application at the bottom. If an agency representative assists you, they will also sign and date the form.
After filling out the form, double-check that all information is correct and that you've attached all required documentation. Submit the form as directed by your local Medicaid office or the instructions provided with the form. By following these steps, you can confidently navigate the process towards securing your healthcare coverage.
Listed Questions and Answers
What is the purpose of the Care 1st Arizona Prior Authorization form?
The Care 1st Arizona Prior Authorization form is designed for individuals with disabilities who are employed, between the ages of 16 and 65, seeking healthcare coverage. It gathers comprehensive information about the applicant, including personal details, employment, income, existing health insurance, and assets, to determine eligibility for Medicaid benefits. The form also facilitates communication needs by inquiring about language preferences, ensuring that interpreter services are provided if necessary.
How can I get help filling out the form if I do not speak English?
If you do not speak English, the form mentions that interpreter services can be provided at no cost to assist with the application process. To access this support, you should contact your local Medicaid office or use the toll-free number provided (1+888+544-7996). For individuals who are deaf or have hearing problems, a specific TTY line (1+800+220-5404) is available for assistance.
What information will I need to provide about my income and assets?
For income, you are required to disclose details about your employment or business, including the total or gross income before deductions and any other sources of money you may have, such as Social Security or retirement pensions. Providing proof, such as pay stubs or tax returns, is necessary to verify your earnings. For assets, you must list all significant holdings you or your spouse may have, including checking and savings accounts, retirement accounts, and property, with necessary proof of ownership and current value.
What happens if I provide false information on the application?
Submitting false information or deliberately withholding information on the Care 1st Arizona Prior Authorization form can lead to serious consequences. This includes potential legal action for fraud, loss of health benefits, and the obligation to reimburse Medicaid for any medical expenses paid out incorrectly. The form emphasizes the importance of providing true and accurate information to the best of your knowledge and outlines the applicant's responsibility to report any changes in circumstances that might affect eligibility.
Common mistakes
Filling out the Care 1st Arizona Prior Authorization form is a crucial step in the process of securing healthcare coverage. However, people often make mistakes when completing this form. Identifying and understanding these errors can help ensure that the application process goes smoothly and increases the likelihood of approval.
-
Not answering every question on the form. The instructions clearly state to fill out every item. Leaving a section blank can lead to delays in processing the application. If the question doesn't apply, it's important to write “none” instead of leaving it blank.
-
Failure to provide proof of income. The form asks for copies of paychecks, tax forms, or other evidence of earnings. Neglecting to send these documents can result in an incomplete application, requiring further follow-up.
-
Incorrectly reporting the number of household members applying for Medicaid. This includes failing to check the box if Medicaid is desired for other members of the household, which can affect eligibility and coverage.
-
Not specifying the preferred language for communication. This form accommodates English, Spanish, Vietnamese, and other languages. Failing to specify can lead to communication barriers and potential misunderstandings during the application process.
-
Forgetting to sign and date the application. An unsigned application is considered incomplete and cannot be processed until this crucial step is completed.
-
Overlooking the need to send proof of other health insurance or Medicare, if applicable. Applicants must include information about any current health insurance coverage, including the insurance company name and policy number.
Avoiding these common mistakes can significantly expedite the approval process and help applicants receive the healthcare coverage they need without unnecessary stress or delay.
Documents used along the form
When navigating the process of seeking healthcare coverage, particularly for individuals with disabilities who work, using the Care 1st Arizona Prior Authorization form is just the beginning. This important document ensures that necessary medical services are approved before they are provided, which is crucial for managing healthcare expenses efficiently. However, to complete this process thoroughly and effectively, several other documents and forms often accompany the Prior Authorization form. Understanding these additional documents can significantly streamline the application process and ensure a more comprehensive approach to securing health coverage.
- Proof of Income Documentation: This includes recent pay stubs, self-employment tax returns, or other evidence of income. It's essential for verifying the income you reported on your application, which helps determine your eligibility and coverage level.
- Proof of Citizenship or Legal Residency: Documents such as a birth certificate, passport, or green card are necessary to prove U.S. citizenship or lawful presence in the country. These documents support the declaration of citizenship or legal residency status made on the Prior Authorization form.
- Medical Documentation: Records or letters from physicians, specialists, or other healthcare providers that detail your current health status, medical history, and the justification for requested services or treatments. This is crucial for establishing the necessity of the services for which authorization is being requested.
- Proof of Other Health Insurance: If applicable, insurance cards, policy documents, or coverage statements from other health insurance must be included. This is to ensure coordination of benefits and to ascertain that Medicaid is the payer of last resort.
- Asset and Resource Documentation: Bank statements, property deeds, vehicle registrations, and similar documents verify assets and resources, impacting eligibility, especially for programs sensitive to applicants' financial situations.
- Disability Documentation: If applying under a disability status, documentation from the Social Security Administration (SSA) regarding SSI or Social Security Disability Insurance (SSDI) benefits, or detailed medical records supporting the disability claim, are necessary.
- Identification Document: A state-issued ID, driver’s license, or other government-issued photo identification helps verify identity and prevent fraud within the application process.
Collecting and submitting these documents, alongside the Care 1st Arizona Prior Authorization form, is a pivotal step toward securing the necessary medical services and support. Each piece of documentation plays a unique role in painting a complete picture of the applicant's situation, ensuring that decisions regarding healthcare coverage are made accurately and fairly. Thus, it's important for applicants to not only understand but also to accurately fulfill the requirements associated with each document to facilitate a smooth and successful application process.
Similar forms
Similar to the Care 1st Arizona Prior Authorization form, the Medicaid Application Form is used to apply for Medicaid healthcare coverage. It includes sections where applicants provide personal information, household details, income, and insurance coverage, much like the Care 1st form solicits details about the applicant’s employment, income sources, and existing coverage. Both forms play a crucial role in determining eligibility for health services, requiring accurate and comprehensive information from the applicant to ensure proper assessment and provision of benefits.
The Disability Benefits Application shares similarities with the Care 1st form, particularly in sections related to declaring a disability and providing details about one’s medical condition and healthcare providers. Like the Care 1st form, it is designed for individuals seeking assistance due to disability, necessitating detailed information about the nature of the disability, treatment, and care providers to evaluate eligibility for benefits. It emphasizes the verification of disability status and the applicant’s need for support, highlighting the importance of detailed medical information in the application process.
The Health Insurance Marketplace Application is another document that bears resemblance to the Care 1st form, especially in the sections where applicants must disclose their income, household composition, and existing health insurance coverage. This form is used for applying for insurance coverage through the marketplace, determining eligibility for premium tax credits and other savings. Much like the Care 1st form, it requires detailed financial information to assess the applicant's eligibility, underscoring the financial aspects of accessing healthcare services.
Lastly, the Supplemental Security Income (SSI) Application has parallels with the Care 1st Prior Authorization form, particularly in areas where applicants are asked about their income sources, assets, and disability status. This form is crucial for individuals with limited income and resources who are aged, blind, or disabled, and seeking financial assistance. Both forms necessitate a thorough disclosure of financial and medical information to evaluate eligibility for assistance, underlying the critical role of detailed personal information in supporting those in need.
Dos and Don'ts
When completing the Care 1St Arizona Prior Authorization form, there are several important practices to follow in order to ensure the process goes smoothly and accurately. Paying close attention to both what you should and shouldn't do will help in avoiding common mistakes and potentially expedite the approval of necessary healthcare services. Here is a list of dos and don'ts:
Things you should do:- Provide accurate and complete information: Make sure all the details you enter are correct. If a section does not apply to you, write "none" to acknowledge you have seen and considered it.
- Include supporting documentation: When the form asks for proof, such as paycheck stubs or copies of tax forms for self-employment, ensure these are attached. Documentation serves as verification of your earnings and can help to process your application faster.
- Use additional sheets if necessary: If the space provided is insufficient for any of your answers, don't hesitate to attach separate sheets with the required information, making sure they are clearly labeled and linked to the main form.
- Indicate your preferred language accurately: This ensures that you will receive assistance or correspondence in a language you best understand, facilitating better communication.
- Sign and date the form: An unsigned form is often considered incomplete. Ensure that both the applicant and if applicable, the agency representative, sign and date the form.
- Report any changes within 10 days: As stipulated at the end of the form, it is crucial to inform Medicaid about any significant changes to your situation. This helps in maintaining the accuracy and validity of your coverage.
- Avoid leaving blanks: If an item doesn't apply to you, write "none" rather than leaving it blank. This shows that you didn't overlook the question.
- Do not provide false information intentionally: False declarations can lead to fraud charges and the possibility of having to repay benefits received erroneously.
- Resist the temptation to guess: If you're uncertain about an answer, it's better to seek clarification than to provide potentially inaccurate information. Incorrect data can result in processing delays.
- Don't forget to attach necessary documentation: Missing documents can stall the process. Ensure all required proof is included when you submit the form.
- Do not wait until the last minute to submit the form: Timely submission is essential. Take note of the date by which the agency needs to receive your application to protect your application date.
- Do not ignore instructions for additional information: At times, the form may request that you contact your local Medicaid office or use a toll-free number for assistance. Neglecting these instructions can lead to errors in your application.
Misconceptions
When navigating healthcare paperwork, the Care 1st Arizona Prior Authorization form often becomes a topic of conversation, alongside a series of misconceptions. Here's a clearer look at the most common misunderstandings:
- It's only for Medicaid applicants. While it primarily serves those applying for Medicaid, it’s designed to facilitate healthcare access for persons with disabilities who work, between the ages of 16 and 65.
- Language barriers prevent application. The form makes provisions for non-English speakers by offering interpreter services at no cost, making the process inclusive.
- Help is hard to find. Assistance is readily available through local Medicaid offices or the provided toll-free number, ensuring support is at hand for those who need help filling out the form.
- You must disclose your race. Providing information about your race is entirely optional. This piece of data is not mandatory for the form's completion.
- Spousal information is always required. You only need to give your spouse's Social Security number if they are also applying, protecting their privacy.
- Proof of Social Security or Unemployment income is necessary. The form states you do not need to send proof of Social Security or Unemployment income, easing the documentation process.
- Medicaid is the only focus. While applying, you can express interest in receiving information about other Medicaid coverage, indicating the form’s role in broader healthcare application processes.
- Income details are irrelevant. You must show the amount of gross income before deductions, providing a clear picture of your financial situation.
- Assets are overlooked. The form requires detailed information about assets or resources, emphasizing the thorough assessment of an applicant's financial state.
- Everyone knows how to access it. Awareness of the Medicaid Purchase Plan and how to apply is not universal. The form concludes with a section asking how you found out about the plan, highlighting efforts to understand and possibly improve outreach.
Clearing up these misconceptions encourages a smoother application process. By understanding exactly what is required, applicants can approach this essential step with greater confidence and efficiency.
Key takeaways
Understanding the Care 1st Arizona Prior Authorization form is crucial for ensuring that individuals with disabilities who are working get the healthcare coverage they need. Here are key takeaways to keep in mind when filling out and using this form:
- Complete all sections of the form accurately. It's important to fill out every item on the form. If an answer is "none" or "0", it should be clearly stated as such. Incomplete or inaccurately filled-out forms may delay the application process.
- Language assistance is available. For applicants who do not speak English as a first language, interpreter services can be provided at no cost. This ensures that all applicants can accurately complete the form and fully understand the Medicaid process.
- Proof of income and resources is required. Applicants need to provide evidence of their earnings, including copies of paycheck stubs, tax forms for self-employed individuals, and other relevant documents. Additionally, information about other income and assets, including savings accounts, retirement accounts, and property, must be verified with supporting documents.
- Information about health insurance coverage is needed. If an applicant has Medicare or other health insurance, details about the coverage and proof of premium payments should be provided. This helps determine the extent of Medicaid coverage required.
- Rights and responsibilities must be acknowledged. By signing the form, applicants confirm that the information they have provided is accurate and understand the consequences of providing false information. They also agree to notify Medicaid of any changes in their circumstances, underscoring the importance of maintaining current and accurate information.
Proper completion and understanding of the Care 1st Arizona Prior Authorization form are essential steps toward securing healthcare coverage for eligible individuals with disabilities. By following these key takeaways, applicants can navigate the process more smoothly and ensure they receive the benefits they are entitled to.
Discover Common PDFs
Arizona New Hire - Make the most of the resources available at the Arizona New Hire Reporting website for an efficient reporting experience.
Arizona Filing Requirements - This form is used to request the Arizona Department of Revenue to waive penalties for reasonable causes.
Arizona Tax Forms - Construction contractors must pay special attention to the bonding requirements section of the JT-1 form, which details the prerequisites for obtaining a Transaction Privilege Tax license.